
Rotator Cuff Tear Surgery in St. Louis
Rotator cuff tears are a leading cause of shoulder pain and dysfunction in the United States. When these patients have failed conservative treatment, arthroscopic rotator cuff repair has become increasingly common for rotator cuff tear treatment. Despite the increasing incidence of rotator cuff repair surgery, failure due to retear remains a significant challenge with reported rates ranging from 11% to 94% in the orthopedic literature. Further, there has been an exponential increase in the number of publications and research interest in treating rotator cuff disorders over the past two decades, however, retear rates and surgical outcomes have remained about the same. Many factors have been identified as affecting retear rates, including patient age, tear size, fatty infiltration and atrophy of the muscles, smoking, and diabetes. Given these factors, tendon biology has been evaluated as a modifiable risk factor for optimizing rotator cuff tear treatment.
More recently, various patches have been used to augment rotator cuff biology, including xenograft, synthetic grafts, allografts, and autograft tensor fascia lata. The use of the long head of the biceps tendon as an autograft has been previously described. More recently, Dr. JT Tokish at the Mayo Clinic in Phoenix developed a novel technique for preparing the graft with a compression device (Figure 1) that also maintains the structural integrity of the tendon, while preserving tenocyte viability. Dr. Duerr completed fellowship with Dr. Tokish, and also spent time this past summer learning this biceps autograft augmentation technique. One of the primary advantages of the biceps autograft is that this is a local graft, and a biceps tenotomy or tenodesis is often performed in conjunction with rotator cuff tear surgery and the remaining portion of the biceps is typically discarded. Not only is this the patient’s own tissue, but it is no additional cost versus other graft options which can cost in the tens of thousands of dollars.
Given Dr. Duerr’s experience with Dr. Tokish and this technique, he was able to be the first surgeon in St. Louis with access to this device and has performed several of these procedures since it was released in February 2023. Dr. Tokish’s early results are promising and Dr. Duerr plans to join the prospective study to follow his own results here in St. Louis.
-
 Figure 1: Biceps tendon removed after subpectoral biceps tenodesis with a 2.7 cm piece being compressed with the compression device.
Figure 1: Biceps tendon removed after subpectoral biceps tenodesis with a 2.7 cm piece being compressed with the compression device. -
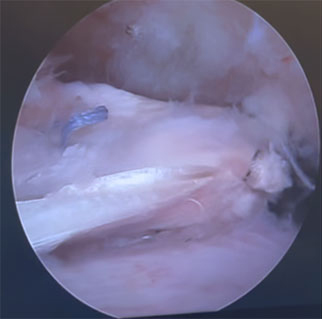 Figure 2: Arthroscopic image of biceps autograft patch being inserted
Figure 2: Arthroscopic image of biceps autograft patch being inserted
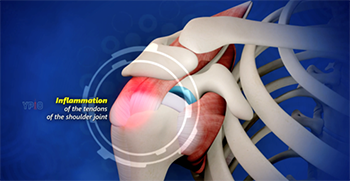 Figure 3: Subacromial impingement with bursitis, or inflammation of the bursa overlying the rotator cuff tendons
Figure 3: Subacromial impingement with bursitis, or inflammation of the bursa overlying the rotator cuff tendons
Rotator Cuff Strain Versus Tear
Shoulder pain and rotator cuff pain occur on a spectrum of disease. Without an acute injury, rotator cuff pain can begin as subacromial impingement with bursitis, or inflammation within the bursa overlying the rotator cuff. This can lead to dysfunction of the bursa and tendinopathy or internal degeneration of the rotator cuff which can cause increased rotator cuff strain leading to pain. This can become chronic and may eventually progress to partial full thickness tearing of the rotator cuff even without any acute injury.
Learn More:
https://www.robertduerrmd.com/shoulder-impingement-orthopedic-surgeon-st-louis-mo/
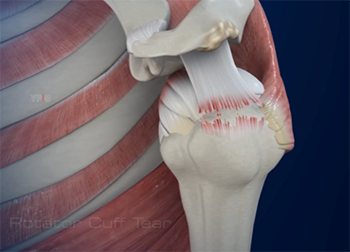 Figure 4: Full thickness rotator cuff tear of the supraspinatus tendon.
Figure 4: Full thickness rotator cuff tear of the supraspinatus tendon.
If there is an acute injury, this can also lead to a spectrum of pathology including a strain of the rotator cuff, which can be intrinsic damage to the tendon without tearing. Rotator cuff tears can range from small partial tears to large or even massive full thickness rotator cuff tears depending on the size of the tear and the number of tendons involved. A rotator cuff tear vs strain differs in that there is actual separation of the tendon from its attachment to the bone on the humerus, or a mid-substance tear within the tendon can occur when there is disruption of the tendon itself.
Learn More: https://www.robertduerrmd.com/rotator-cuff-tear-orthopedic-surgeon-st-louis-mo/
Rotator Cuff Tear Treatment
Rotator cuff tears are treated many ways depending on the cause of the tear (chronic versus acute or traumatic tear), size and location of the tear, and a number of patient-related factors such as age, smoking status, occupation and activity levels.
Rotator cuff strain vs tear is treated conservatively with:
- Rest, Ice, Compression
- Home exercise program (See below)
- Physical Therapy
- Anti-inflammatory medications
- Subacromial steroid injection
Rotator cuff tear treatment is similar to a strain initially with the above conservative treatments. If these treatments fail to provide adequate relief, surgery sometimes is indicated. Dr. Duerr performs all of his rotator cuff repair surgeries with a minimally-invasive arthroscopic approach. This enables a faster recovery with less damage to the surrounding muscle and less pain after surgery. Learn more about rotator cuff repair surgery: https://www.robertduerrmd.com/rotator-cuff-repair-orthopedic-surgeon-st-louis-mo/
Rotator Cuff Tear Exercises
There are a number of exercises that can be done to preserve shoulder range of motion, maintain and build strength of the rotator cuff and surrounding muscles. There are 17 muscles that attach to the scapula or shoulder blade including the 4 rotator cuff muscles. When one of these muscles is injured, it can lead to a cascade of abnormal scapular movement that can lead to pain and dysfunction in any of these muscles that attach in this area. Here are just some of the rotator cuff tear exercises that you can do on your own:
Range of motion exercises:
- Pendulum swings
- Posterior shoulder stretch
- Doorway stretch
- Sleepers stretch
Strengthening exercises
- Internal rotation
- External rotation
- Abduction (T-shape)
- Bent over rows
- Overhead press
- Upright rows
- Bench press (Barbell and Dumbbell)
- Incline bench press (Barbell and Dumbbell)
- Decline bench press (Barbell and Dumbbell)
- Push ups
- Pull ups
- Weighted pull downs
Please note, if you do not have experience with these exercises, I would recommend working with a physical therapist or trainer before beginning any weight lifting regimen.
Rotator Cuff Recovery After Surgery
After surgery, you will be wearing a sling for 4-6 weeks. The first 24 hours after surgery, you will be immobilized in a sling and a shoulder-specific ice machine will be provided. On the day of surgery you will also have a nerve block which will provide pain relief for the first 12-24 hours. Once the block wears off, you can begin some gentle pendulum exercises.
Please note that these are general guidelines and Dr. Duerr has very specific protocols depending on the size of your tear and your specific needs. So please follow the specific protocol that he will assign on the day of surgery or at your initial post-operative appointment.
Day 1 – 14 (Healing Phase):
- You will be wearing the sling full time. You may remove the sling for pendulum exercises and hygiene only. You may shower on the 3rd day after surgery. I recommend sleeping in a recliner chair, or if you have a bed that elevates the head or can use pillows to create a ramp to sleep with the shoulder elevated well above heart level.
- You will have your first follow-up appointment around 10-14 days after surgery and we will assess the incisions and will plan to start your physical therapy after this visit. *Unless Dr. Duerr has placed you in the Accelerated protocol, which should begin PT within 5-7 days after surgery.
Weeks 2 – 6 (Initiate physical therapy (PT) Phase):
- You will begin physical therapy and they will start with gentle passive range of motion exercises
- The goal of this phase to progress to near full range of motion with the physical therapist moving the arm for you
Weeks 6 – 12 (Range of motion Phase)
- Phase II of physical therapy will progress with active range of motion exercises (ability to lift your arm on your own)
- You will also begin isometric exercises in this phase and the physical therapist will continue with other modalities as needed (e.g. ice, e-stim, heat)
Weeks 12 – 18 (Strengthening Phase)
- During this phase you will begin gentle resistance exercises as directed by your physical therapist with bands or light weights
Weeks 18+ (Return to Activities Phase)
- Depending on your activity level and your goals, you may begin progressing back to some higher impact activities and begin sports-specific rehab at this time.
- Typically throwing will not begin until 6 months post-surgery
Helping Local Patients
Dr. Duerr joined Mercy in August, 2022, and hopes to bring his experience and expertise to patients in the St. Louis community who may be candidates for rotator cuff repair with biceps augmentation. If you believe you could benefit from a consultation with Dr. Duerr, please reach out to our office for a consultation: Request appointment online.